Quotes from: Compassion-focused therapy as an intervention for sexual offending
| Type of Work | Methodology for therapy |
- This article is published as Chapter 9 in: Forensic Interventions for Therapy and Rehabilitation - Case Studies ans Analysis - Edited by Belkinda Winter, Nicholas Blagden, Laura Hamilton and Simon Scott - Routledge, London, 2022.
- The References age given in a separate RTF file: cft_references.pdf.
- A Dutch version "Citaten uit ..." is given here:
< https://www.helping-people.info/compassie_als_de_kern.html >.
A brief history of sexual offending treatment
Before exploring the benefits of a new approach to working with sexually harmful behaviour, it is necessary to briefly review the history and development of intervention initiatives for sexual offending. [...]
[...] modern treatment for sexual offending has its roots in behaviourism. [...]
Behaviourism understands human behaviour to be a series of responses to the environment via respondent and operant conditioning. These theories were applied to understanding sexual interest and saw atypical sexual interests as resulting from contingency learning, where sexual arousal was paired with another stimuli such as children and then reinforced via masturbation [...].
Treatment approaches were broadly split into [a] those that aimed at reducing arousal to offence-related interest (...) and [b] those that aimed to increase arousal to healthy sexual interest (...).
Evaluation shows some short-term positive gains from these techniques (...); however, behaviourism has been beset by weak research methodologies, using single case designs, with little use of controlled experimental designs (Akins, 2005). A meta–analysis by Furby, Weinrott and Blackshavv (1989) examined 42 studies completed in this era and concluded that there was little or no difference in re–offending among treated and untreated samples.
As cognitive behavioural therapy (CBT) became increasingly dominant in mainstream psychotherapy, interventions for people who commit sexual offences followed suit, and CBT remains the primary approach (Schmuker & Lösel, 2017). This led to an explosion in research and treatment approaches which placed the focus of treatment on changing faulty thinking. [...] Cognitive restructuring became one of the most common components of sexual offending interventions [...]
This era of treatment also saw the use of schema therapy for people with sexual convictions, drawing on research suggesting that schema–driven cognitions interacting with negative life events are causally relevant to sexual offending for some individuals (Mann, 2004). Schemas observed to be relevant to offending were labelled 'dysfunctional’, understood to be acquired via developmental experiences. The therapeutic goal was to reconstruct schemas into functional equivalents.
The concept of relapse prevention was often central to CBT programmes for sexual offending. This focused clients on recognising their relapse cycles, spotting high–risk situations and faulty thinking and deploying strategies to manage these. Avoidance was a common strategy encouraged in the early versions of these interventions. [... ... ...]
The early 2000s saw the introduction of a model of correctional programming that was directed according to risk level and crinrinogerlic need and could respond to individual factors (risk, need, responsivity [RNR]:Andrews & Bonta, 2003). [...] the top three most reported intervention tagets for residential and community programmes were [a] offence responsibility, [b] social skills training and [c] victim empathy. [... ... ...]
Despite meta–analyses indicating gains in reducing recidivism, the outcomes for interventions are not universally positive; some interventions show iatrogenic effects (e.g. higher recidivism rates for the intervention than the comparison group) (Mews, Di Bella & Purver, 2017). Clearly some interventions work for some individuals; however, the question about what works for whom and when remains elusive.
An important question in sexual offending interventions is how they are delivered. For example, some interventions may be delivered in a manner that stimulates shame (Levenson, 2014); however, shame has been implicated as an inhibitor to engagement in therapy and behaviour change
- (Tangney, Stuewig & Hafez, 2011; Walton, 2019)
A further consideration is that outcomes in the prevailing research have focused on recidivism, and very few studies measure or report client wellbeing as an outcome worthy of note. This is a feature of sexual offending intervention that sets it apart from its mainstream psychotherapy counterparts, where client wellbeing is considered to be a primary reason for intervention.
The focus on risk and risk reduction as the primary ethos for the intervention of people who offend was questioned by Ward (2002) in his Good Lives Model (GLM) of rehabilitation. The GLM’s inherent assumption is that people are not inherently pathological and that all human behaviour has an evolutionary function.
Understood in this context, offending is considered to be motivated by the pursuit of unmet human needs. For example, a person may commit a sexual offence against a child in the pursuit of the need for emotional connection and sexual reward (Laws & Ward, 2011). Intervention therefore should aim to equip individuals with the skills to achieve these needs in pro–social ways. The GLM emphasises the importance of addition, not elimination, which is the need to work towards developing strengths and capabilities rather than eradicating problematic factors, a mainstay of many interventions for sexual offending. [...]
The GLM represents a significant evolution in thinking about sexual offending and the response to it, depathologising in favour of emphasising individuals’ strengths. [... ...]
Early outcomes for interventions which have incorporated GLM suggest that it is as good as an established relapse prevention intervention in bringing about change (Harkins et al., 2012) and seems to reduce attrition (Ward & Willis, 2013) [...] GLM offers a promising overarching rehabilitation framework and points towards a more humanistic and person–centred approach as a useful focus for contemporary offence work. [...]
After decades of research on the effectiveness of interventions for sexual offending, the inconsistent outcomes suggest that like psychotherapy generally, current approaches are only helpful for some people some of the time (Gloster et al., 2019). This points to need for a range of interventions to cater for varying need and a move away from a 'one size fits all’ approach.
Trauma, adversity and the evolution of criminogenic need
As we have seen in the previous section, there have been various incarnations of interventions for sexual offending. [...] These various incarnations have a recurring theme that the individual is perceived as intrinsically faulty, whether that be due to deviant arousal pathways, distorted patterns of thinking or skill deficits. In essence, the assumption is that the people who receive treatment are different, not just as determined by their actions but by something that renders them fundamentally different from others.
[... ...] the emphasis has been on individual pathology, an approach that is likely to stimulate shame (and a sense of maladaptation), enhance a pathological identity (self as deviant, distorted, etc.) and lower self-esteem.
We argue that a formulation of the origins of criminogenic need is critical to effective intervention and that an absence of such a consideration may not only neglect predisposing factors but may reinforce the circumstances that evolved these factors.
[... ... ...] In our opinion, and indeed in our experience, developing an awareness of the function of criminogenic factors is essential to effective therapeutic practice and supports people who have these capacities to develop effective management strategies without the burden of shame.
An exploration of the impact of trauma and early adversity offers some insight into why this may be the case. The relationship between early trauma and later life difficulties has been widely documented thanks in part to the Adverse Childhood Events (ACE) research programme (Felitti et al., 1998).
[...] An exploration of the impact of trauma and early adversity may offer some insight into the links between life experiences, learning and harmfulness. [...]
The first paper to emerge from the ACE research identified a clear association between seven categories of adverse early experiences and a broad range of later–life difficulties, including alcoholism; suicide; drug use; depression; and physical health difficulties such as heart disease, cancer, lung and liver disease (Felitti et al., 1998).
Since the publication of Fehtti’s initial paper, there has been a plethora of studies further examining the links becween childhood adversity and difficulties later in life. ACEs have been linked to increased experiences of
- anxiety and depression (Merrick et al., 2017), to
- dissocidtive strategies such as psychosis (Varese et al., 2012),
- increased likelihood of drug and alcohol dependency (Strine et al., 2019) and
- disruptions to personality development (DeLisi et al., 2019).
It is perhaps unsurprising that studies have also revealed an association between these harmful experiences and offending (harmful) behaviour. In terms of general offending rather than specific offence types, numerous studies have pointed towards an association between early adversity and offending in later life [... ... ...].
Of particular note in the context of early trauma and chronic adversity is the significance of shame. Shame has been cited extensively as a repercussion of trauma, abuse and maltreatment (Shahar, Dorn & Szeosenwol, 205). [...] There seems to be a general consensus that shame is a self–conscious emotion that leaves us feeling judged as a consequence of a transgression or wrongdoing [...]
As we will see later, from a compassion–focused perspective, shame, like other emotions, is understood in terms of its evolutionary function whereby it motivates us to manage ourselves in order to avoid such judgments and social rejection. [...]
We argue that where shame has been prompted by early trauma, it stimulates adaptive responses and builds our capacity to use these responses throughout life.
The information that has emerged from the various ACE studies cited earlier points towards the role of trauma and adversity in the genesis of criminogenic need and the interruption of various developmental trajectories, including relational abilities, empathy, social responsibility and psychological wellbeing. These abilities to regulate emotions, sustain affiliative relationships, mentalise and empathise, acknowledge responsibility and feel guilt are all areas of human functioning that have, at various incarnations of intervention for sexual offending, been primary targets.
Although the salience of these areas has changed over time, a trauma–informed understanding may facilitate greater insight into how the interruption of these capacities may increase criminogenic vulnerability. In turn, an understanding of this vulnerability can orientate forensic practitioners to consider interventions that are explicitly sensitive to the trauma that may have impacted on the development of compassion and the sensitivity towards suffering of others that can appear to be absent in the actions of those who commit offences.
Trauma-informed interventions
[... ...]
In light of the growing evidence for trauma prevalence in the histories of people who sexually offend, Levenson and Grady (2016) suggest that CBT [Cognitive Behavior Therapy] interventions for sexual offending should take account of the research on trauma, attachment and developmental psychopathology in the approach and response to individuals. They highlight the need to explore and recognise the underlying origins of dynamic risk for individuals to understand how trauma experiences have shaped their lives and linked to offending. A means of achieving this is to move towards trauma–informed intervention models (Levenso, Willis & Presscott, 2017). Viewed in this way, psychological characteristics related to sexual offending (dynamic risk factors) can be understood as adaptive and understandable responses to threatening life situations.
Trauma–informed care therefore is not an intervention in itself, but a framework for delivering intervention that takes account of the traumatic underpinnings of criminogenic need and promotes safety, trust, choice, collaboration and empowerment at the core of the interaction (Levenson, 2017).
[... ... ...]
We suggest a combination of a trauma–informed approach with CFT to create trauma–informed and compassion–focused practice can offer a model of intervention for those who commit serious harm.
Compassion-focused therapy
CFT was initially developed for people whose high levels of shame rendered them unable to benefit from traditional C[ognitive]B[ehavior]T[herapy] (...). C[ompassion]F[focused]T[herapy] is a motivation–focused therapy that helps people to access and stimulate the affiliative emotions, motives and competencies underpinning compassion. The combination of these capacities plays an important role in threat regulation, wellbeing and pro–social behaviour (Gilbert, 2014; Clapton. 2016).
In CFT, compassion is conceptualised as a motivation (not an emotion) of two psychologies: [a] a sensitivity to suffering and [b] a commitment to alleviating suffering. Where capacities for this are stimulated, an individual’s motivation is fundamentally shifted towards a caring mentally, directed both at others and oneself. The ability for CFT to stimulate the motivational caring system has obvious benefits for people who harm.
As with many therapeutic approaches, CFT incorporates a number of core components:
1. Psycho-education
provides an overview of the core components of CFT, which outline that the human brain evolved in a way that resulted in certain inbuilt problems, including biases and inherent conflicts, many of which make us vulnerable to anti–social behaviour and mental health problems.
Furthermore, much of what happens in our brains is neither our design nor our intention and as such is not our fault. This is not to invalidate our responsibility for our own actions, but simply to recognise that the architecture of our brain is not something that we choose.
For example, a child who experiences abuse from a parent may learn to deny their experience of abuse in order to retain the important aspects of that relationship (the need for food, shelter, etc.). In so doing, they may train their mind to deny harmful acts and inadvertently lay a foundation from which their own antisocial behaviour can easily emerge.
CFT suggests that the more individuals identify with the problems of common humanity and the troubles of the evolved (and tricky) brain, the less personalised and the easier it is to work with shame and take responsibility for change.
Part of psycho–education also involves helping individuals begin to understand the nature of their different emotion systems and how they can learn to be more physically and mindfully aware, thus enabling people to be more attentive to what is going on in their own minds and bodies as they arise.
In addition, CFT teaches specific breathing exercises (called soothing rhythm breathing) that are designed to stimulate the parasympathetic system, which in turn has an impact on the frontal cortex and capacities for reflective thinking (Lin, Tai & Fan, 2014).
Within forensic CFT, we propose a number of key concepts that should occur early in the therapeutic process:
- The nature of our evolved brain,
- Evolved emotions and emotion regulation systems,
- Compassion,
- Fears, blocks and resistance to eompassion,
- The way our motives organise our attention, thinking, feeling and behaviour, known as 'multiple selves’, [and]
- Reconceptualising criminogenic need.
2. Formulation
is based on the evolutionary model of human nature and aims to help people understand that many of their life strategies for dealing with threats and trying to advance oneself are the consequence of genes interacting with social contexts. Helping individuals to understand the unintended and often unhelpful consequences of their safety or acquisition strategles is therefore important and facilitates a de–shaming process.
Formulation is also a co–production that aims to capture an autobiographical narrative. The formulation is explicitly based on certain key assumptions – that we have an evolved brain and that the way the person presents to us has been shaped by lifetime experiences and therefore represents a functional and survival–based response to their lifetime.
Furthermore, there is an explicit recognition that effective survival responses are inevitably resilient to change (rather than treatment resistant) .
Formulation is also based on a phenomenological rather than categorical understanding and is written in a style that ensures that it rs accessible and available and can be held in mind by the author.
3. In CFT, the development of compassionate motivation
is seen as a core transforming process that arises from insight. There are a range of interventions for building compassion motivation, including
- the use of compassion imagery,
- compassionate reflection,
- compassion–focused empathy,
- developing a compassionate self–identity,
- regular practice of compassion and behaviour and
- keeping compassion diaries (Gilbert, 2010).
It is helpful to recognise that sometimes individuals can practice behaving and thinking in compassionate ways long before they start 'feeling’ compassion.
4. As compassionate motivation is developed,
this capacity can be used to support individuals to grieve for their own distress, and as the ability to experience sadness and vulnerability is developed, they can be supported to develop compassion and remorse for their own harmful actions. Within CFT, it is acknowledged that the capacity for genuine remorse (i.e. a sadness for the harm caused and a feeling of guilt) is unlikely to develop without a capacity for sadness for one’s own distress. Attending to personal trauma is therefore central to the therapeutic process and is woven throughout the process of therapy.
5. Within forensic settings,
CFT also supports people to understand the origins of criminogenic need. By adopting a developmental and phenomenological approach, people can be supported to understand how they acquired or nurtured capacities that may contribute to risk or harmfulness. By tracking the development of criminogenic factors over time, we can support people to recognise the function of criminogenic factors in their original context (typically safety related).
Supporting people to understand the original function can offer a rationale and therefore reduces the potential for shame. Enabling people to see that they needed to disconnect from other people’s feelings (callousness) or that they needed to be ready to react (impulsivity) allows people to begin to address these factors without feeling they were at fault for having them in the first place.
CFT, then, is
a motivation–focused form of psychotherapy and sees the motivational states of mind – whether we want to cause suffering or whether we want to alleviate suffering – as central to working with people who cause harm to others. CFT encourages an understanding that early life experiences may have compromised people’s capacity for caring by over-stimulating the threat system and under–stimulating the soothing system. The effect on self–relating that emerges from early trauma is seen to be a driving feature behind the experience of shame in men and women who cause harm and, similarly, an inhibitor of guilt.
As a psychotherapeutic intervention, forensic CFT adopts a trauma–sensitive approach and recognises that much of what we learn is beyond our control. CFT empowers individuals to take notice of the consequences of their learning and develop their skills and competencies in order to manage themselves in a harm-free manner. CFT encourages compassion-based guilt rather than disempowering shame. Application of CFT as an intervention for offending is novel and has most readily been used an approach for working with those who experience
- anger (Kolts, 2012),
- violence (Taylor, 2017) and, more recently,
- youth in custody (Da Silva et al., 2019).
However, in our view, the ability of CFT to address trauma and shame and to stimulate caring motivations towards others positions it as a promising intervention for those who commit sexual harm (...).
Intervention case examples
In this section, we set out two different interventions that utilise CFT as their primary therapeutic approach. We provide a brief overview of each intervention, drawing together a number of specific considerations for forensic CFT. We
conclude the chapter with a brief summary of early outcome data from the two
interventions.
The Aurora Project for sexual offence prevention
The Aurora Project (TAP) is a community–based group intervention. Beginning in 2018, it aims to help people who experience sexual thoughts and feelings that, if acted upon, would cause harm. TAP is part of a range of interventions offered by the Safer Living Foundation (SLF) charity ( < www.saverlivingfoundation.org/ > to prevent harm caused by sexual offending. The intended client group is those who have not committed a sexual offence, the principle being that first–time offending could be prevented. Only an outline of TAP is provided here, but for a more detailed description see Hocken (2018).
The development of TAP drew heavily on the emerging literature around people attracted to chidren but not having offended [...]. The psychological needs of this group are varied and diverse, but common needs identified are
- coming to terms with their sexual interests (Dombert et al., 2016);
- managing self–hatred, shame and stigma related to their interest (Jahnke & Hoyer, 2013); and
- loneliness, isolation and mental ill health (Grady, Levenson & Bolder, 2017).
These needs set alongside the research indicating that, for some, a sexual interest in children is immutable (Cantor & McPhail, 2016) point to an intervention that builds capacities for self–compassion and acceptance. [...]
TAP utilises two therapeutic modalities:
- C[ompassion]F[ocused]T[herapy and
- Acceptance and Commitment Therapy (ACT), [...].
CFT and ACT work as complementary approaches, and both share the evolutionary model at their core. ACT offers an explicit focus on developing psychological flexibility mediated by mindful awareness, acceptance and values–based living.
T[he]A[aurora]P[roject takes a rolling group format, although clients will have a number of individual sessions in preparation for the group phase and at any subsequent point as needed.
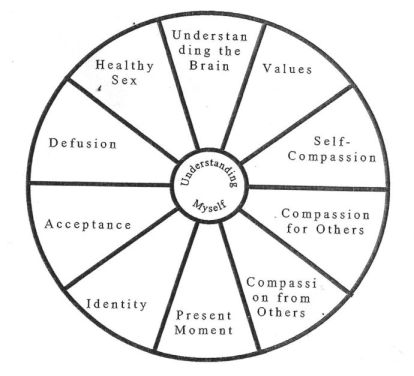
The structure revolves around ten modules which are based on the three flows of compassion (from self to others, from others to self and from self to self) , psycho-education, the core processes of psychological flexibility from ACT and a problem–specific module on healthy sex. The modules and components of Aurora are shown in Table 9.1.
Table 9.1: Components of the Aurora project intervention
- Understanding the brain
Psychoeducation of model – tricky brain, emotional regulation model - Values
Identifying what matters (values) and developing skills and motivation for value–based living - Self-compassion
Fears, blocks and resistances; stimulating a caring motivation towards the self; multiple selves; shame; self-criticism; guilt - Compassion for others
Stimulating a caring motivation towards others, skills for caring behaviours, guilt - Compassion from others
Stimulating a capacity to receive care from others - Defusion
Decentring and skills for meta–cognition (noticing, naming and standing back from internal experiences) - Acceptance
Motivation and skills for acceptance of internal and external experiences - Present moment
Attentional training, grounding, mindfulness, soothing breathing - Identity
Multiple selves, compassionate self - Healthy sex
Skills from the prevlous areas applied to sexual, thinking feeling and behaviour
The modules are not distinct phases, and they are not completed chronologically or exclusively. The concepts from each module are continually referred to and linked to the other modules. For example, where a session is focusing on self–compassion, it will draw on the other areas as relevant. Each client starts with psycho-education in pre–group individual sessions to lay the foundation for the intervention, and they join the group knowing the basic concepts of tricky brain and emotional regulation systems. [...]
The client journey begins with individual assessment with a therapist to explore their needs and undertake assessments that map on to the module areas. Based on this, a regularly reviewed collaborative formulation is developed, which is used to guide the priority need areas the client will focus on. The formulation is conceptualised as a compass, depicted as a circle with ten segmentg containing each module (see Figure 9.1), and the relative need is noted on the compass in some way by the client, typically by drawing a line to show how 'full’ the segnent is.
Figure 9.1: Aurorra life compass formulation
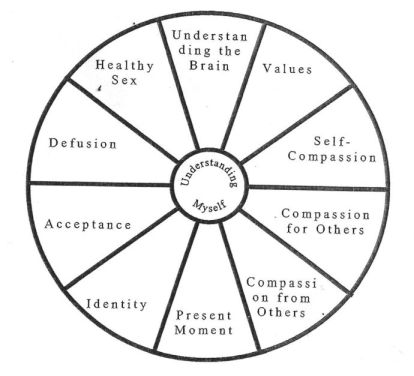
The compass signifies direction, and meeting the needs in each area helps clients move in the life direction they want to go. Sessions are loosely planned around each module, taking into account individual need areas. Participants are also set between session assignments to develop learning and help them generalise this to their daily life. [...]
[...] results are preliminary.
Assessments show that most individuals entering Aurora are experiencing high levels of
- internalised shame,
- depression, anxiety,
- little–to–some hope for the future,
- low mental wellbeing,
- reduced levels of perceived social safety and
- moderate–to–low psychological flexibility .
Preliminaly results show positive changes at 24 weeks into Aurora.
- Mental wellbeing is in the clinically normal range, closer to the average of the general population.
- There is a steep reduction in internalised shame, while depression and stress are also reduced to normal levels.
- In addition to this, there was a statistically significant reduction in anxiety
- Participants also display a greater hope for the future and increased levels of social safety
- Psychological flexibility is largely unchanged.
These are promising results and suggest that, at the least, Aurora is improving the quality of life for participants. [...]
Compassion-focused forensic psychotherapy programme
CFT has been used [...] as an overarching framework to organise work with men in prison for sexual offences who have not been able to respond to the cognitive behavioural interventions. Drawing on the theoretical foundations we have described earlier, the therapeutic work strives to support the men to develop their capacity to feel guilt (and therefore guide their actions away from harmfulness) by supporting them to process their own experiences of adversity and understanding how they have been shaped by experience.
Taking into account our evolved architecture, including our innate readiness to cause harm, and adopting a perspective that 'we learn what we live’, men are supported to provide and experience their own autobiographical formulation as a foundation for subsequent work.
[...] Emotional regulation is [...] unlikely to be successful if emotional dysregulation was learned as a survival strategy in other words, we need to establish a foundation before we try to build skills or competencies that support resilience and desistence. [...] We have conceptualised the work within a sequence (see Table 9.2) .
Table 9.2 Trauma–sensitive forensic CFT
Module/phase -- Components
- Psycho-education
Therpeutic objectives: Evolved minds and tricky brains; evolved emotional regulation system; compassion; multiple selves; fears, blocks and resistances. - Mindful compassion
Concurrent module that runs across the programme: Soothing rhythm breathing; attention training; mindfulness; visualisation; self–compassion. - Formulation
Autobiographical narratives; formulating a good life. - Trauma sensitivity
Psychoeducation (how we respond to trauma); creating a trauma–informed understanding; facing trauma (compassion for our life story, emotional mirroring, offence trauma) . - Understanding criminogenic need
Origins of criminogenic need; criminogenic need in current context; witnessing consequences. - Facilitatting guilt
Understanding harm caused; mentalising the people we harm; practicing guilt, restorative commitments.
[...] The men at Whatton are serving prison sentences and have therefore been convicted of causing harm. The programme therefore explicitly addresses criminogenic capacities and aspires to operate as a risk–reducing intervention. As such, there is a module that addresses harmful capacities, including directly criminogenic areas such as
- sexual interests,
- sexual preoccupation and
- values that promote harmful behaviour.
In addition, less direct characteristics that can contribute to harm, such as
- difficulties in accepting responsibility,
- externalising blame
- and accountability and an indifference to suffering,
are also included in order to ensure a broad context for intervention.
Men are encouraged to lead on the development of a formulation of their harmful behaviour by contextualising the origins of their criminogenic needs within their personal life story. [...] The bulk of the intervention is trauma focused, and this then forms a basis that allows men to develop insight into the origins of their criminogenic need and the function or purpose of these as they emerged. [...]
Having developed a compassionate understanding of the initial function of chIninogenic factors, the therapeutic work moves to develop insight into the harmful repercussions of these factors. [...]
It is considered important that this does not start until individuals have developed the capacity for self–compassion and a clear understanding of how their learning experiences have influenced their ways of relating to others. [...]
Within CFT, the aspiration here is that people can now visit this work, having developed both the competencies and the motivations for compassionate and pro–social behaviours. [...]
Considerations in forensic CFT
As we can see from Figure 9.1, 1ike many psychotherapies, CFT starts by socialising the client to the model. We have added to the content of this module over time (on the basis of client feedback) and alongside the psychoeducational work we aim to set the tone for the work. In other words, we teach the core components of CFT with compassion, with a willingness and a sensitivity to noticing distress and a genuine intention to alleviate suffering.
There is also a constant balance between delivering content and responding to processes in the room. As we have said, the bulk of the therapeutic work is trauma (in its broadest sense) and adversity focused, and we draw heavily on trauma–focused CFT, which is described in elegant detail elsewhere (Lee & James, 2012). As we have developed our practice, we have been eager to learn from the men (primarily) who have endeavoured to work in this way, and we have become aware of some particularly nuanced aspects of forensic CFT that are worth attention.
Process issues
First, despite the vast array of psychotherapies, almost all are united in the assumption that the therapist wants the client to improve for himself or herself. Carl Rogers’ (1957) notion of the core conditions for therapy offers a scaffold for the development of a containing relationship that allows people to disclose information about themselves.
[... ....]
Creating a psychotherapeutic culture (acceptance, validation, compassion and curiosity) is therefore the first step when we commence this work in forensic settings.
Second, by drawing attention to the nature of the relationships in the therapy room, we create opportunities to explore social processes and dynamics. [...] In the context of forensic practice understanding the algorithms (stimulus–response rules) that orchestrate our different motivational systems seems particularly pertinent. [...]
Similarly, knowing why and how someone recruits the various behavioural repertoires of a rank–based mentality may shed light on a need for dominance and thus may also be central to understanding and managing the risk of further harmful behaviour.
Third, by introducing social processes into the scrutiny of therapeutic work, we can begin to explore these as they emerge, particularly within the therapeutic relationship (see Figure 9.2).
Figure 9.2: The dynamic of a therapeutic alliance
- Parental relationship
↓ - Attachment style:
Secure - Anxious - Ambivalent - Disorganised
↓ - Reltional patterns
↓ - Theraperutic relationship:
Transference - Counter-transference
In other words, we can explore the transferences the feelings and attitudes held about and between different members and facilitators of the group – and what this may reveal about earlier relationships and their influence on current relating styles. Exploring this in the context of C:FT, where we understand the influence of evolution and learning, allows us to depersonalise and de–shame the therapeutic relationship.
Brain architecture (tricky brain)
The concept of a tricky brain is a central aspect of CFT. In essence, the idea is that the basic architecture of the human brain leaves us vulnerable to a range of difficulties – including those that are often described as psychiatric or criminogenic. From the experience that we have gained from working with CFT in forensic settings, three aspects of the evolved and tricky mind concept stand out.
First, evolved brains allow us to recognise that much of what happens in our minds is not a result of our own design and therefore not our fault. We have found that a critical issue here is understanding a shift from a stance that advocates blame and shame into one that encourages guilt and responsibility [... ...]
[...] We encourage people to notice what they are and what they are not responsible for and therefore what they can begin to develop more control over.
If we consider the issue of sexual interests, the blame/shame stance suggests that sexual interests are wilfully and inevitably pursued, while the guilt/responsibility position recognises that we do not choose our sexua1 preferences [...], but we can consider the consequences of our interests if we choose to pursue them or not.
The second area of difficulty here concerns life experiences and learning. [...] A sexual interest in children may be understood in terms of genetic influences, and this level of understanding often allows people to separate blame and responsibility. [...]
However, where our presentation is based on learning and experience, this can be trickier, and we have often been greeted with statements like “so it’s not my fault [...]" or “ I’m not to blame for [...]”.
Clearly, we would not endorse this perspective, but would again encourage people to notice what is, and what is not, their responsibility [... ... ...].
Finally, a third area that may need some attention can arise when our clients have
experienced abuse or hurt in their earlier lives and they mistake the idea of a tricky brain to mean that the person who caused them harm is also not responsible for their actions. As discussed earlier, this can quickly prompt questions directed towards the therapist along the lines of “so you’re saying it is not his fault he used to batter me every time he got drunk” or “so I guess it was my fault I got raped”. As we have already indicated, this is absolutely not what we are suggesting, and these understandable reactions allow us to emphasise the distinction between fault and responsibility. However, this sort of interaction also allows the compassion–focused therapist to invite their client to explore the therapeutic alliance, including the therapist’s thoughts and feelings towards the client and vice versa.
Formulation
While formulation is a common aspect of all psychotherapies, many forensic formulations have become organised around risk factors and, in some formats, have gradually become a risk diagnosis – a tick box of criminogenic symptoms. As with all aspects of this work, an awareness of risk is clearly important, but the evolutionary understanding of human development that sits at the heart of CFT recognises both the phylogenetic (evolution over time) and ontogenetic (evolution over a life span) influences on human behaviour.
To enhance phenomenological experiences and embody trauma sensitivity, we invite clients to begin a formulation with the phrase “when I was little . . .” and find that this helps us to orientate this process towards their own autobiographical experience of life. For many people who have spent time living within forensic settings, this can prove challenging. [... ... ...]
However, we argue that the aim of a formulation process is to enhance understanding and support someone to develop insight into their own human nature. Furthermore, the ownership of a formulation should rest with the person who it describes, and ownership is clarified with a first–person narrative account.
Criminogenic need in an autobiographical context
Criminogenic need has been an important construct that has enhanced our understanding of the types of factors, characteristics and lifestyle choices that may increase the likelihood of harmful behaviour. However, interventions that seek to address these various factors rarely support clients to understand the biological and genetic origins of our behaviours, nor how these behaviours come to be cultivated over the course of our life. Understanding criminogenic need in these ways can therefore stimulate shame and encourage a range of shame management strategies that we have referred to previously.
The CFT approach to formulation that we have outlined earlier provides a different understanding of criminogenic challenges because it allows us to witness the evolution of these factors across the developmental period. As indicated in Table 9.2, the formulation is followed by trauma–focused work where we are able to understand the childhood survival strategies that were necessary.
As we move into this phase of the work, we begin to turn attention to the manifestation of these strategies in adulthood and support a person to notice the unintended consequences that may have arisen from trauma responses. “What are your risks and where did they come from?” is a phrase developed by one of the groups that worked to this model and allowed them to understand their lack of agency as these various factors came into being, whilst encouraging their responsibility to develop strategies to manage, contain or inhibit harmful capacities.
Conversely, however, embedded within this understanding is the notion that we cannot un–learn and therefore we are not able to leave behind those aspects of ourselves that can be harmful. Understanding the significance of trauma, adversity and the need to develop ways to survive these conditions helps to illustrate the challenge in this.
Language acquisition can be a useful metaphor at this stage. [... ...]
In terms of harmfulness[...] we have to learn ways to manage these aspects of ourselves and new adaptive ways of meeting the needs these old harmful behaviours once met.
This can challenge previous interventions where the concept of old me / new me was used as a metaphor for risk management. We have found that a person who has invested in the old me concept can be reluctant to acknowledge that they still possess the capacity to be harmful and can experience some distress (or anger) as we encourage them to turn towards this aspect(s) of themselves.
Facilitating guilt (compassion for others and compassion for my victims)
[... ... ...]
In CFT we see compassion as the key motivation that will enable our clients to turn towards the distress that they can cause and strive to alleviate suffering. In other words, we are facilitating the experience of guilt. [...]
After reflecting on the work with the people who have been willing to undertake it, two areas have been experienced as particularly challenging at this stage of the work.
- [1] The first refers to balancing feelings of guilt with shame, while
- [2] the second is linked to the grief that arises when guilt is experienced and the barriers to restoration in relation to victims.
[1 - The first area]
In terms of the balance between these two emotions [guilt with shame], we have been helped understand that many people who cause serious harm to others experience shame and are therefore motivated (by shame) to seek to regain status and social acceptance. In turn, various behaviours (denial, rationalising, seeking forgiveness, etc.) facilitate this process and protect the individual from having a deep understanding of the harm that they have caused. For many of the men we have worked with, shame has become a practiced emotion and one that can readily be used.
Our balance to this is to invite responsibility by encouraging these individuals to recall times when they have caused minor harm or distress to others. [...]
Having processed their own experience of being harmed and having grieve for their own losses associated with this, men can turn towards the distress that they have caused and experience the grief that they have caused. Inevitably, this is a challenging area of work and rests both on the capacity for the men to cultivate compassion and on the quality of the therapeutic relationships.
[2] The second area...
... that causes challenges for the men involved in our work concerns the experience of repair. Compassion involves both noticing and wanting to relieve distress, and the evolution of guilt has rooted behavioural change into the process of harm reduction.
When our own actions have caused such considerable harm as to prevent us from talking to our victim(s), the opportunity for direct reparation is blocked. We have learned that this can create a fracture in the experience of compassion (including guilt), as men may be left feeling expose to the harm that they have caused and motivated to alleviate suffering but unable to do so.
As guilt involves a behavioural component that is designed to reduce suffering, we have drawn on the concept of redemption scripts (Manrna, 2001) as a framework to support men to identify compassionate lifestyles that evidence a commitment to be “helpful not harmful” (Gilbert, 2020).
Conclusion
The development of trauma–aware practice demonstrates the prevalence of adverse child experiences in the histories of people with sexual offences and points to functional links between trauma and sexual offending. However, common feature of the predominant intervention models is a focus on criminogenic needs without attention to the (often traumatic) genesis for these.
We have argued here that survival responses to trauma and adversity give rise to the development of criminogenic needs, and it is necessary to address the origins of criminogenic factors in order to prevent further harm. We propose that CFT offers a therapeutic model for doing this, providing a means to formulate criminogenic needs in the context of trauma and a means of developing a motivation that moves people away from harmful behaviour. The two case examples of interventions that use CFT as their main component show promising outcomes for psychological wellbeing and acknowledgment risk.
References
The References age given in a separate RTF file: cft_references.pdf.
{kind=link}